Diletta Vittoria Carla Settimi*
Unicamillus University, Italy
Corresponding Author:
Diletta Vittoria Carla Settimi, Unicamillus University, Italy
Abstract
Introduction: Retroperitoneal fibrosis (RPF) is a rare fibroinflammatory disorder characterized by progressive deposition of dense collagenous tissue within the retroperitoneal space, encasing vascular and visceral structures. Although most cases are idiopathic, certain pharmacological agents have been implicated in symptom exacerbation. This case report describes an acute deterioration of gastrointestinal function following initiation of a non-selective beta-adrenergic blocker in a patient with otherwise stable disease.
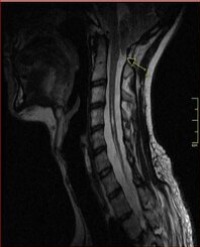
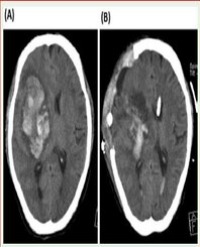
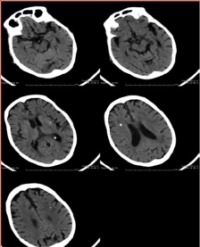
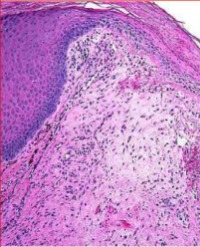
Case Presentation: A 45-year-old Caucasian woman with dyslipidemia and chronic sinus tachycardia underwent exploratory laparotomy for suspected peritoneal malignancy. Histopathological examination confirmed extensive fibrotic deposition with chronic inflammatory infiltrates and excluded neoplasia, establishing a diagnosis of RPF. During three years of surveillance with serial laboratory testing and magnetic resonance imaging, the disease remained quiescent. To optimize heart rate control, therapy with a beta-1-selective antagonist was replaced by propranolol 40 mg twice daily, a non-selective beta-adrenergic blocker. Within days, she developed severe crampy abdominal pain, marked distension, and altered bowel habits, despite stable imaging findings. The close temporal relationship, together with the established role of beta-2 receptors in intestinal smooth muscle relaxation, implicated non-selective blockade in aggravating colonic dysmotility against a background of fibrotic compression. Dietary modifications and low-dose antispasmodics provided only marginal relief.
Conclusion: This case highlights that non-selective beta-blockers may exacerbate gastrointestinal symptoms in RPF by impairing smooth muscle relaxation. In patients with colonic involvement, beta-1-selective agents should be preferred, with careful consideration of cardiovascular benefits versus gastrointestinal risks.